

For more than a century, radioactivity has been used in oncology for both diagnosis and treatment. In diagnostics, one of the best-known tools is fluorodeoxyglucose-positron emission tomography (FDG-PET). FDG is a glucose-like molecule labeled with a small amount of radioactive fluorine-18. Due to cancer cells consuming large amounts of glucose, FDG can help visualize metabolically active tumors during a PET scan1. As therapy, radiation was one of the first, and still most commonly employed cancer treatments. An external beam directs high-energy x-rays towards the tumor, with the overall goal to destroy cancer cells while minimizing damage to surrounding healthy tissue2.
Over the past 10-15 years, a newer approach has moved into the spotlight. Instead of aiming radiation from outside the body, new treatments involve the delivery of radiation directly to cancer cells from within3.
The new era of targeted radiopharmaceuticals
Targeted radionuclide therapy (TRT) uses radiopharmaceuticals, a new treatment approach that combines the molecular precision of targeted therapy to selectively deliver a pay load to cancer cells, with the killing or visualization effects of radiotherapy. Most radiopharmaceuticals have three main parts: a radioactive isotope, a linker, and a targeting molecule (Figure 1a). Like LEGO® pieces, each part can be changed depending on the application, the target, and the goal of treatment. Together, these three parts influence how well the drug reaches the tumor, how specifically it binds to cancer cells, how long it stays in the bloodstream, and how quickly it clears from the body4.
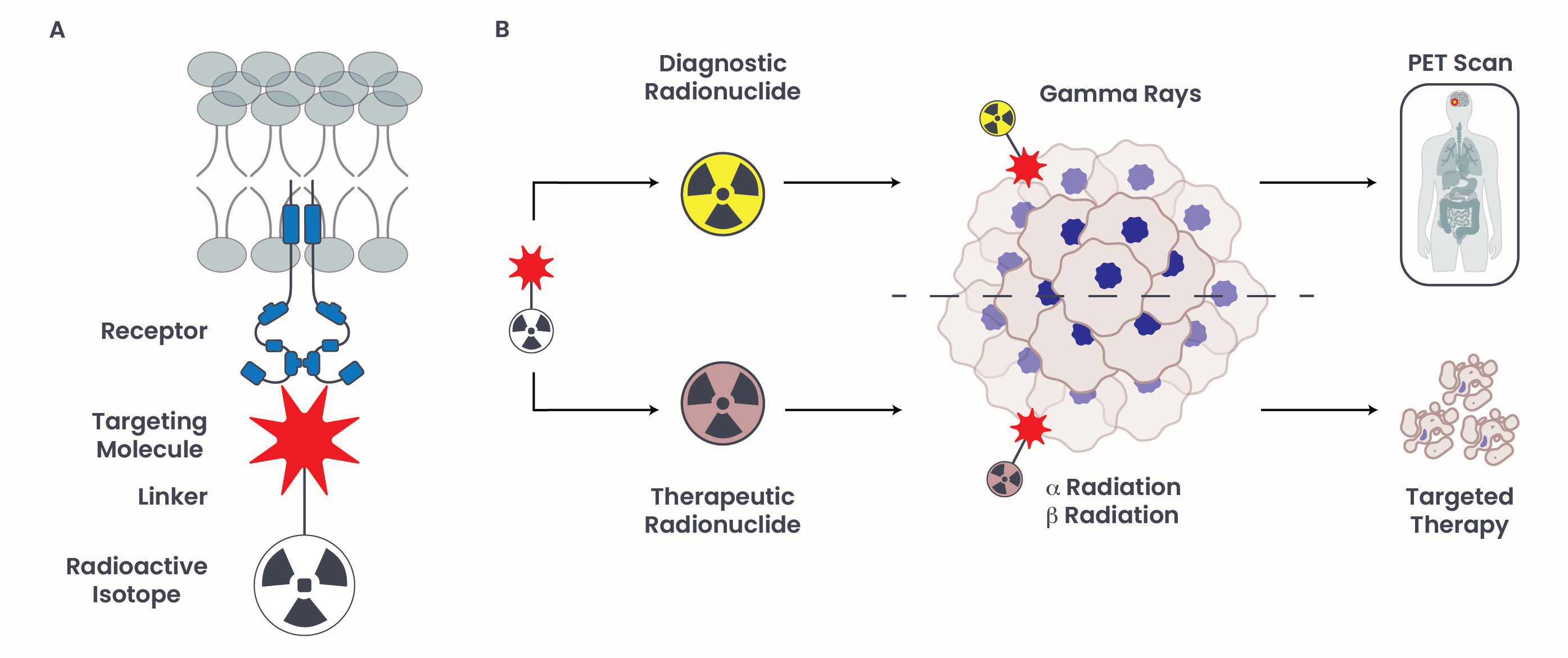
Figure 1. Targeted radionuclide therapy and their use in diagnosis and treatment of cancer.
The radioactive isotope is the radiation-emitting payload. Different isotopes are used for different purposes. Some are best suited for imaging, while others are used for treatment (Figure 1b). Imaging agents most often use isotopes that emit gamma particles that penetrate most materials and can be detected by scanners, such as in PET, but do not do significant damage to DNA. Therapeutic agents usually emit beta- or alpha-particles, which are capable of damaging DNA and thereby killing cells. Alpha particles travel only a very short distance in tissue, but they release a large amount of energy along that path. Beta particles travel farther than alpha particles and can affect not only the targeted cell but also nearby cells.
The linker connects the radioactive isotope to the targeting molecule. Although it may look like a simple bridge, the linker can strongly affect how stable the drug is in the bloodstream, how long it remains near the tumor, and how quickly the unbound drug clears from healthy tissue.
The targeting molecule is the biologically active molecule guiding the radiopharmaceutical to the target cancer cells. The specific cells can be identified by a marker, such as a receptor protein found at high levels on the surface of certain cancer cells. Once a TRT finds and binds to its target, it may stay on the cell surface or be internalized into the cell. The radioactive isotope then constantly releases DNA-damaging radiation, resulting in cell death when near DNA where it can cause the most damage.
The “see and treat” approach
Radiotheranostics, the combination of diagnostic with therapeutic radiopharmaceuticals, is often described as a “see and treat” approach (Figure 2)5. The “see” step uses an imaging radiopharmaceutical to confirm that a patient’s tumors express a specific marker. This helps clinicians identify patients who are most likely to benefit from a matching therapeutic radiopharmaceutical. This approach is often referred to as patient stratification, where a treatment is chosen based on the presence or absence of a relevant biological signature. Unlike a single-site tissue biopsy, which samples only one tumor location, imaging provides a noninvasive whole-body molecular characterization of the expression of a specific receptor throughout the body. This is especially helpful when cancer has spread to multiple sites, because primary tumor and distant metastasis might not always express the same markers. The “treat” step uses a therapeutic radiopharmaceutical that recognizes the exact same targeting molecule but carries a radioactive isotope designed to damage cancer cells. The “see” part can also continue during and after treatment. Follow-up imaging may help clinicians understand whether tumors are responding, whether disease is progressing, or whether target expression is changing over time.
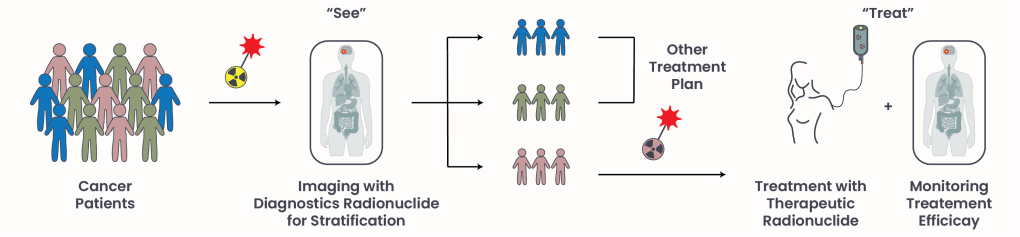
Figure 2. The “see and treat” approach.
Two of the best-established FDA-approved radiotheranostic treatment areas are gastroenteropancreatic neuroendocrine tumors (GEP-NETs) and metastatic castration-resistant prostate cancer (mCRPC). Currently, there are two therapeutic pharmaceuticals and their corresponding imaging counterpart FDA-approved (Table 1): Lutathera ([177Lu]Lu-DOTATATE) and Pluvicto ([177Lu]Lu-PSMA-617)5.
Lutathera6 ([177Lu]Lu-DOTATATE) | Pluvicto7 ([177Lu]Lu-PSMA-617) | |
|---|---|---|
| Manufacturer | Novartis Pharmaceuticals Corporation | Novartis Pharmaceuticals Corporation |
| Radioactive isotope | Lutetium 177 | Lutetium 177 |
| Radioactive decay | ꞵ radiation | ꞵ radiation |
| Targeted patient population | Neuroendocrine tumors affecting the digestive tract (GEP-NET) | Metastatic PSMA-positive, castration-resistant prostate cancer (PSMA+ mCRPC) |
| Targeting molecule | Somatostin receptor (SSTR): Hormone receptor commonly overexpressed on the vast majority (about 90-92%) of neuroendocrine tumors (NETs) | Prostate-Specific Membrane Antigen (PSMA): Heavily overexpressed on the surface of cancer cells in 90% of metastatic prostate cancer patients |
| Initial FDA-approval | 2018 | 2022 |
| Approval based on | NETTER-1 trial (NCT01578239) | VISION trial (NCT03511664) |
| Most common adverse events | Nausea, diarrhea, and abdominal pain | Fatigue, dry mouth, and nausea |
| Imaging counterpart | [68Ga]Ga-DOTATATE [64Cu]Cu-DOTATATE | [68Ga]Ga-PSMA-11 |
Table 1. Radiotheranostic agents approved for cancer treatment.
Future Direction
Although radiotheranostics have been proven to be a powerful tool for rapid imaging and effective elimination of tumor cells, they remain a second- or third-line option in clinical practice. Researchers are now testing whether radiotheranostics may be more effective when used earlier in the course of disease or in combination with other cancer treatments8.
Additionally, several challenges remain. Disease-targeting molecules for FDA-approved radiopharmaceuticals are limited and come with off-target radiation, poor clearance from the body and impaired clinical response due to the high variability in target expression. Those limitations are currently being addressed in ongoing clinical trials. Scientists are developing new targets, better linkers, improved carrier molecules, and different sources of radioactivity. The goal is to increase radiation delivery to tumors while reducing exposure to healthy tissue.
For patients, the promise of radiotheranostics is both practical and personalized: it offers a way to visualize the cancer, choose treatment based on what is actually present in the body, and deliver radiation with greater precision.
- American Cancer Society (7 May 2025). PET Scan for Cancer. https://www.cancer.org/ Retrieved 24 May, 2026 from https://www.cancer.org/cancer/diagnosis-staging/tests/imaging-tests/nuclear-medicine-scans-for-cancer/pet-scan.html. ↩︎
- American Cancer Society (9 Jun 2025). Radiation Therapy. https://www.cancer.org/ Retrieved 24 May, 2026 from https://www.cancer.org/cancer/managing-cancer/treatment-types/radiation.html. ↩︎
- Primac I, Tabury K, Tasdogan A, Baatout S, Herrmann K. The molecular blueprint of targeted radionuclide therapy. Nat Rev Clin Oncol. 2025 Nov;22(11):869-894. doi: 10.1038/s41571-025-01069-z. Epub 2025 Sep 9. PMID: 40926013. ↩︎
- Gandhi N, Alaseem AM, Deshmukh R, Patel A, Alsaidan OA, Fareed M, Alasiri G, Patel S, Prajapati B. Theranostics in nuclear medicine: the era of precision oncology. Med Oncol. 2025 Sep 26;42(11):498. doi: 10.1007/s12032-025-03061-0. PMID: 41006727. ↩︎
- Tran HH, Yamaguchi A, Manning HC. Radiotheranostic landscape: A review of clinical and preclinical development. Eur J Nucl Med Mol Imaging. 2025 Jun;52(7):2685-2709. doi: 10.1007/s00259-025-07103-7. Epub 2025 Feb 1. PMID: 39891713. ↩︎
- Novartis Pharmaceuticals Corporation. (Feb 2026), START STRONG WITH LUTATHERA. https://www.novartis.com/. Retrieved May 24 2026 from https://www.lutathera-hcp.com/. ↩︎
- Novartis Pharmaceuticals Corporation. (Feb 2026), STRIVE EARLIER FOR PLUVICTORY. https://www.novartis.com/. Retrieved May 24 2026 from https://www.pluvicto-hcp.com/. ↩︎
- Lapi SE, Scott PJH, Scott AM, Windhorst AD, Zeglis BM, Abdel-Wahab M, Baum RP, Buatti JM, Giammarile F, Kiess AP, Jalilian A, Knoll P, Korde A, Kunikowska J, Lee ST, Paez D, Urbain JL, Zhang J, Lewis JS. Recent advances and impending challenges for the radiopharmaceutical sciences in oncology. Lancet Oncol. 2024 Jun;25(6):e236-e249. doi: 10.1016/S1470-2045(24)00030-5. PMID: 38821098; PMCID: PMC11340123. ↩︎
© 2025 WithinOncology. All rights reserved.
This article, including all text, tables, and figures, is the intellectual property of WithinOncology and its contributors. Unauthorized reproduction, distribution, or use of any content without explicit written permission is strictly prohibited. For inquiries, please contact us via the contact form.

Leave a comment