

“A healthy person wants a thousand things, a sick person only wants one” – Confucius
Health is something we often take for granted—until we don’t have it anymore. While we do our best to keep healthy, the false sense of security good health provides us often results in inadequate self-care. According to an early detection survey conducted by the Prevent Cancer Foundation in 2024, nearly seven out of 10 U.S. adults are behind on at least one routine cancer screening1. Late cancer diagnosis increases the risk of late-stage cancer diagnosis and poorer treatment outcomes. The primary reasons for missing out on available cancer screenings include lack of awareness about the need for screening (43%), the absence of family history (38%), and not experiencing any symptoms (33%). This gap in proactive cancer screening means that many cancers are detected at advanced stages, when treatment options are more limited and less effective. Early detection is crucial, as it significantly improves survival rates by catching cancers or their precursors before they have progressed. Despite the immediate need for improved detection, the scope of current screening methods is narrow and focused only on a limited number of cancer types, only detecting one at a time (Table 1). The need for improved methods of early detection is underlined by the fact that 70% of all cancer-related deaths are due to cancers that currently lack screening tests.
| Type of Cancer | Cancer Screening |
|---|---|
| Breast Cancer | Mammograms |
| Cervical Cancer | Pap Tests and HPV Tests |
| Colorectal Cancer | Stool Tests and Colonoscopy |
| Prostate Cancer | PSA Blood Test |
| Lung Cancer | Low dose CT Scans |
Table 1. Current cancer screening methods.
Today, novel methods for early detection of cancer are the subject of intense research – much of which is beginning to prove fruitful. Emerging cancer tests have the potential to simultaneously screen for multiple types of cancer. Rare and hard-to-detect cancers can also now be detected, as well as those with poor prognoses. The best time to treat cancer is early but detecting it before symptoms present is a significant challenge. Luckily, novel tests can also signal the presence of cancer before symptoms appear. Multi-cancer early detection (MCED) tests currently in development offer a promising advance.
MCED tests offer the advantage of broad detection through a single, minimally invasive blood test. Research over decades has revealed that cancers shed DNA, called circulating tumor DNA (ctDNA), and proteins, into the bloodstream (Figure 1). Proteins and ctDNA originating from cancers are called ‘cancer signals’. Cancer signals help to distinguish healthy from cancerous cells and identify the presence and potential origin of a tumor before symptoms appear.
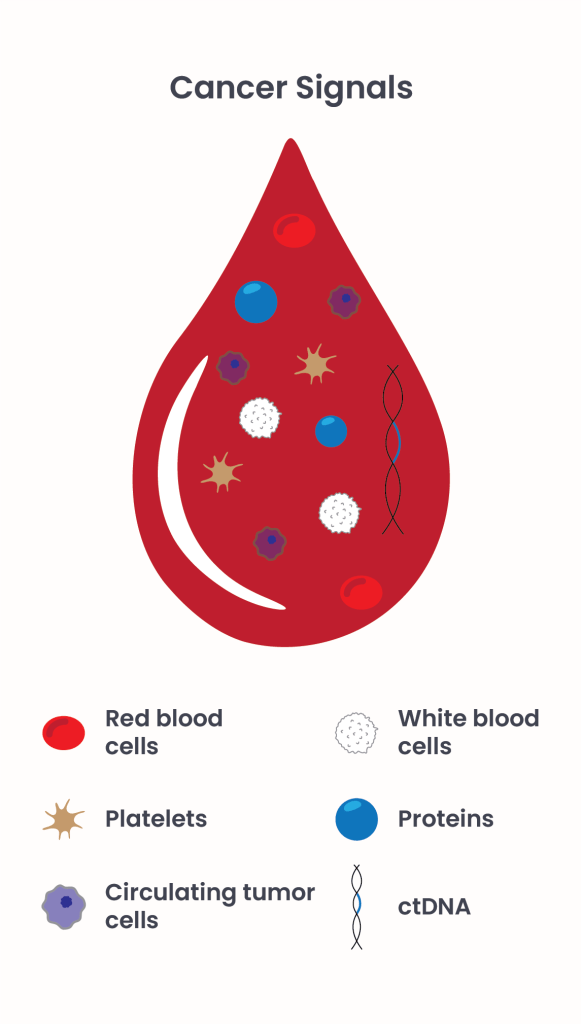
Figure 1. Individual components within our blood.
Promising MCED Tests: A Closer Look
The quality of MCED tests in the following described clinical trials is characterized and improved based on two major parameters: Specificity, the ability to distinguish between healthy and cancerous cells, and sensitivity, the ability to detect even low cancer signals.
Galleri2 by GRAIL
GRAIL has developed a blood-based test called Galleri, that screens for ctDNA only, and can detect over 50 different types of cancer. The test is certified under the Clinical Laboratory Improvement Amendments (CLIA) program, which allows the testing of human samples in GRAILs laboratory only. Galleri is recommended for adults with an elevated risk for cancer, such as those age 50 or older, and is available by prescription only. The current price for this test is $949 and is not covered by most insurance plans.
Two significant studies underscore the potential of the Galleri test:
- The Circulating Cell-free Genome Atlas study3 (CCGA; NCT02889978) was a case-controlled observational study that enrolled approximately 15.000 participants, both with and without cancer, to develop and validate a MCED test. Results indicated a high specificity of 99.5%. The test’s sensitivity improves with disease progression: it identifies 16.8% of stage I cancers but detects 90.1% of stage IV cancers. In addition, it was also able to predict the organ of origin responsible for the cancer signal with an accuracy of 88.7%.
- The PATHFINDER study4 (NCT04241796) is an interventional study investigating the feasibility of broad implementation of the Galleri test in 6621 participants. The study demonstrated a high sensitivity of 99.5% and an 88% accuracy in identifying the cancer signal origin. Importantly, 71% of the cancers detected by the Galleri test were types for which no standard screen test exists, and 48% of these were stage I-II. This highlights the Galleri test’s potential to significantly impact early detection, especially for difficult-to-detect cancers.
Cancerguard5 by Exact Sciences
Cancerguard is a blood-based test designed to screen for multiple cancer signals, enabling the early detection of various types of cancer. The test is not FDA-approved yet and solely available through participation in clinical trials.
Two key studies highlight its potential:
- Detecting cancers Earlier Through Elective mutation-based blood Collection and Testing study6 (DETECT-A) was an exploratory, prospective, and interventional study enrolling 10,000 women (ages 65 to 75) with no prior history of cancer. The study evaluated the feasibility and safety of integrating a blood-based cancer screening test into routine clinical care, focusing on surgically treatable cancers with curative intent. Participants underwent the blood test CancerSEEK, an early version of Cancerguard, alongside standard screening tests to detect cancer and positron emission tomography–computed tomography (PET-CT) to localize the site and extent of the disease. While the blood test detected 26, standard screening tests detected additional 24 cancers, resulting in the detection of 96 cancers in 10 different organs. Importantly, the blood test identified early-stage cancers as well as cancers lacking standard-of-care screening test, reinforcing its potential value in routine clinical care.
- Ascertaining Serial Cancer patients to Enable New Diagnostic 2 study7 (ASCEND-2) is a large, multi-center, prospective, case-control study of over 11,000 participants aged 50+ with known cancer and healthy controls. The MCED test achieved an overall sensitivity of 50.9% with 98.5% specificity. Importantly, it has a sensitivity of 63.7% for the 6 most aggressive cancer organ types with the shortest 5-year survival rate.
Despite their potential to be a huge milestone for the health system, MCED tests are not meant to replace current cancer screening tests rather than being complementary to current standard screening to advance early detection. Thus, limitations like the following are currently addressed:
- Detection of early-stage cancer: Early-stage cancers are often small and release a lower amount of cancer signals into the blood, making them even harder to detect.
- Test accuracy: No test is perfect. MCED tests may incorrectly classify a proportion of people either as having cancer (false positive) or not having cancer (false negative). In addition, it could overdiagnose cancer that wouldn’t cause harm.
- Follow-up requirements: After a positive result additional diagnostics are necessary to confirm the cancer’s location and type.
- Cost: Blood-based cancer screening test are not covered by most health insurance plans.
Thus, improvements are still needed to enhance MCED tests’ sensitivity for early-stage cancers and to minimize false results. Although no MCED test has received FDA approval yet, significant progress is being made, and several promising candidates are emerging.
MCED tests like Galleri and Cancerguard represent a critical step forward in cancer screening, providing hope for earlier detection and improved outcomes. However, their role will be complementary to traditional screening methods, emphasizing the importance of a comprehensive approach to cancer prevention and early diagnosis.
- Prevent Cancer Foundation. (1 Apr. 2024), U.S. adults are still behind on routine cancer screenings—but reasons why vary by race. Kevin Kuzminski. Retrieved February 1 2025 from https://preventcancer.org/news/u-s-adults-are-still-behind-on-routine-cancer-screenings-but-reasons-why-vary-by-race. ↩︎
- Galleri. (n.d.) Go further with cancer screening. Retrieved February 16 2025 from https://www.galleri.com ↩︎
- Nadauld LD, McDonnell CH 3rd, Beer TM, et al. The PATHFINDER Study: Assessment of the Implementation of an Investigational Multi-Cancer Early Detection Test into Clinical Practice. Cancers (Basel). 2021;13(14):3501. doi:10.3390/cancers13143501. ↩︎
- Klein, E.A. et al., Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set., Annals of Oncology, Volume 32, Issue 9, 1167 – 1177. ↩︎
- Exact Sciences. (n.d.), THE ERA OF MULTI-CANCER EARLY DETECTION IS JUST BEGINNING. http://www.exactsciences.com. Retrieved February 16 2025 from https://www.exactsciences.com/science-pipeline/cancerguard-multi-cancer-early-detection ↩︎
- Lennon AM, Buchanan AH, Kinde I, et al. Feasibility of blood testing combined with PET-CT to screen for cancer and guide intervention. Science. 2020;369(6499):eabb9601. doi:10.1126/science.abb9601. ↩︎
- Exact Sciences. (8 Apr. 2024), EXACT SCIENCES TO PRESENT LATE-BREAKING DATA FROM ASCEND-2 STUDY VALIDATING ITS INVESTIGATIONAL MULTI-CANCER EARLY DETECTION TEST AT AACR ANNUAL MEETING 2024. http://www.exactsciences.com. Retrieved February 16 2025 from https://www.exactsciences.com/newsroom/press-releases/exact-sciences-to-present-late-breaking-data-from-ascend-2-study ↩︎
© 2025 WithinOncology. All rights reserved.
This article, including all text, tables, and figures, is the intellectual property of WithinOncology and its contributors. Unauthorized reproduction, distribution, or use of any content without explicit written permission is strictly prohibited. For inquiries, please contact us via the contact form.

Leave a comment